
SLEEP LINK:
Electronic devices emit blue light which delays melatonin. This can cause a change in the sleep pattern and shift the body’s natural clock (also known as the circadian rhythm) later.
Caffeine is a stimulant. Therefore, both excess caffeine use and use late in the day (within 6 hours before bed) can disrupt the ability to fall asleep and stay asleep due to the central nervous system effects of this drug.
Parental Involvement is important to monitor both caffeine and electronic device use in addition to setting and enforcing bedtimes. While a major reason teens are not getting enough sleep is due to early school start times, instilling teenagers with these healthy “sleep hygiene” techniques aid in ensuring healthy sleep practices.
Electronic Devices
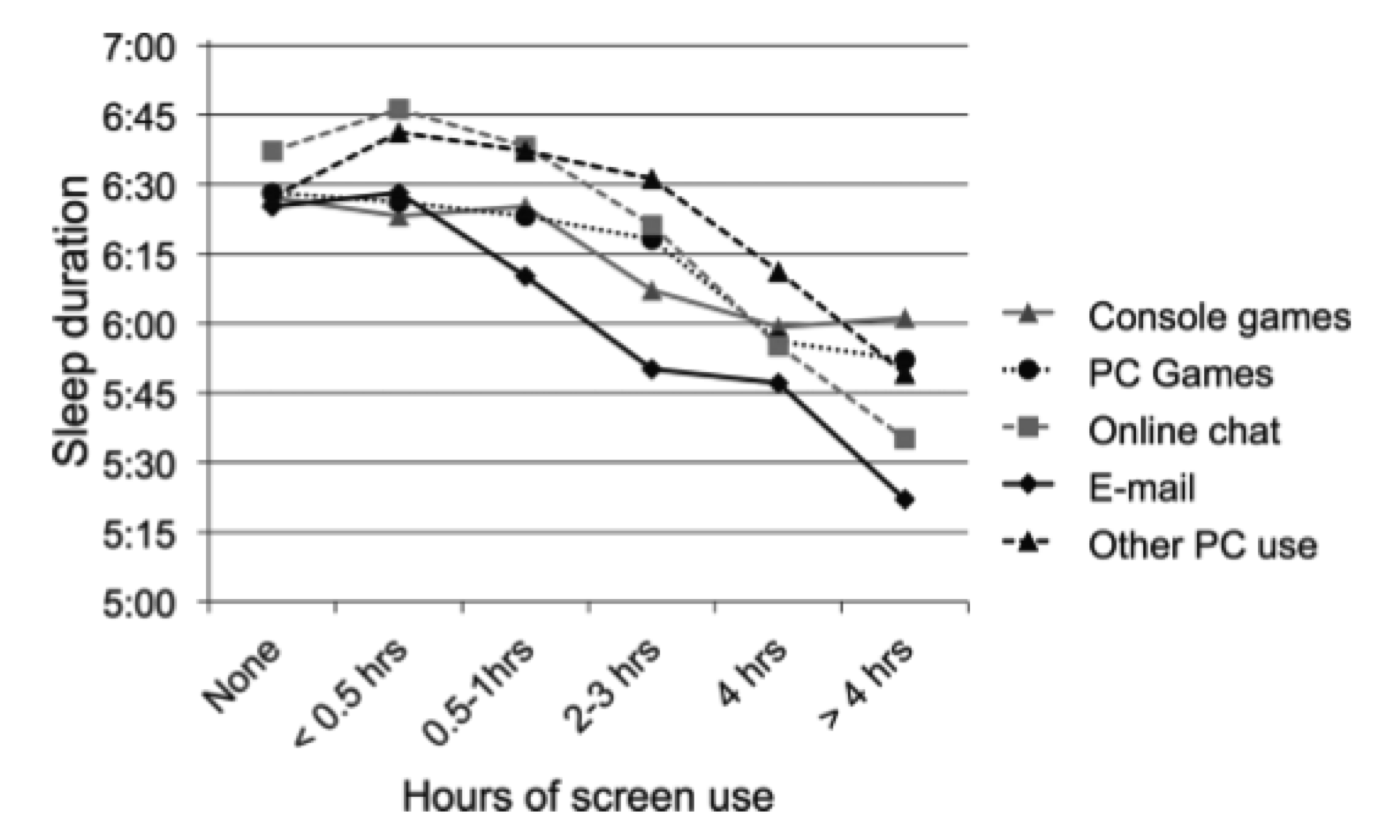
80-90% of adolescents use a smart phone within 1 hour of bedtime, which can negatively impact the ability to fall asleep leading to a decrease in the amount of sleep acquired. The more time a child spends in front of a screen directly impacts the quantity of sleep they receive. (Graph 1) (1)
Graph 1:
Caffeine
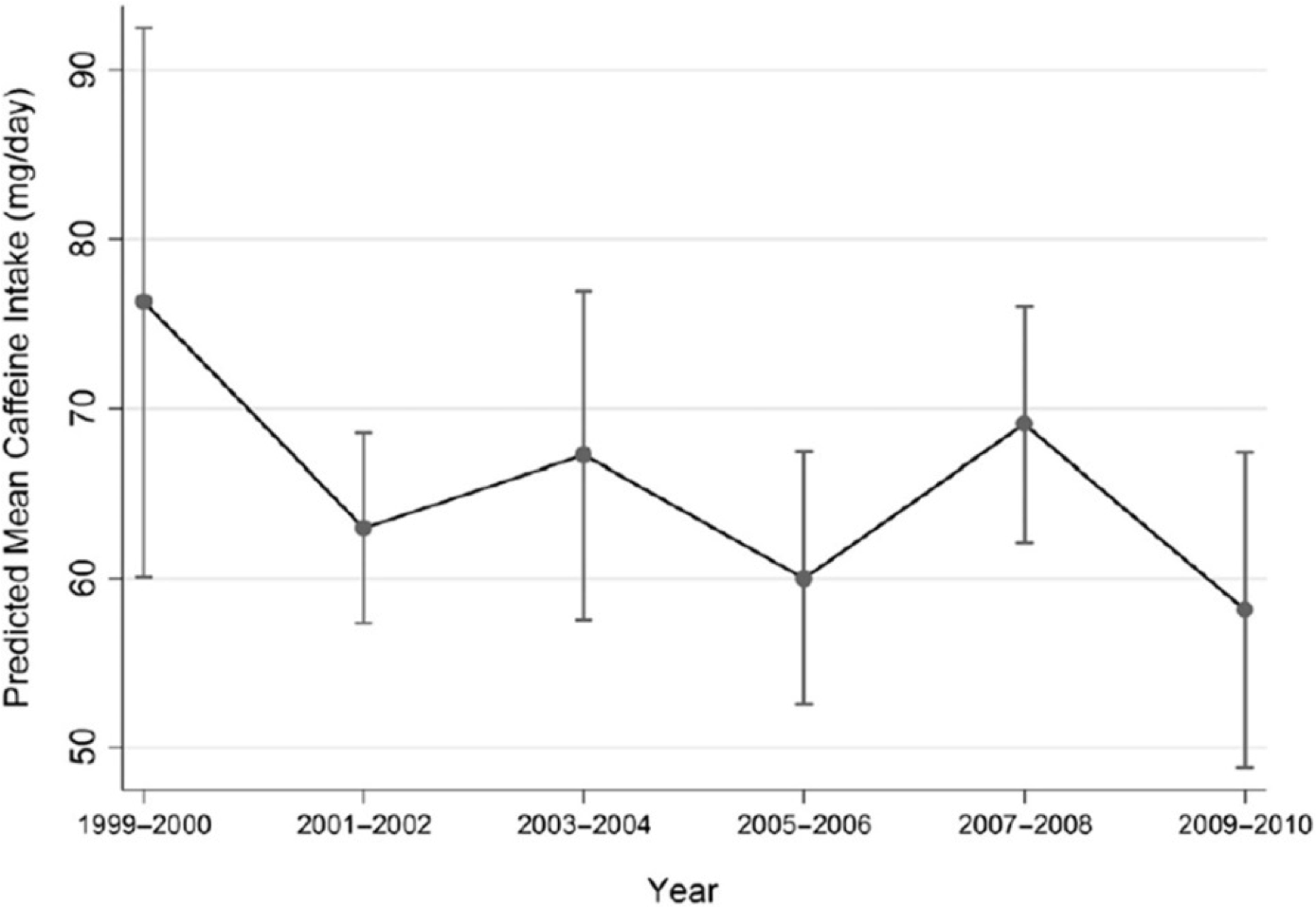
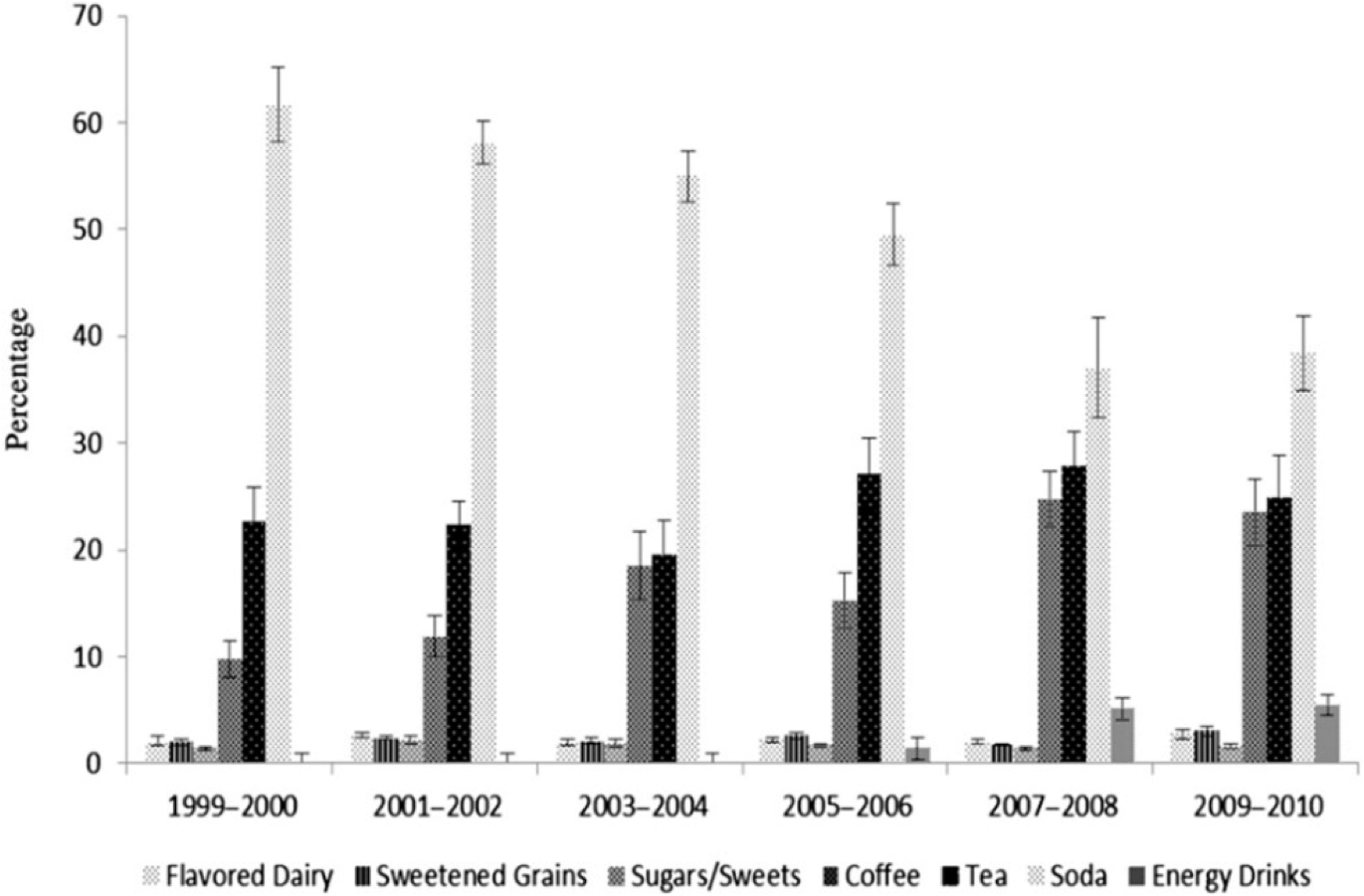
While consumption of caffeine has decreased in the past decade (Graph 2), the consequences of caffeine use in childhood is raising concerns. Soda and tea have been replaced by the availability and sales of energy drinks, specialty coffee drinks, and food products containing caffeine, including candy bars, potato chips, and gum. Consumption of these products has dramatically increased over the past decade and products are often marketed toward children and adolescents (Graph 3). (2)
Graph 2:
Graph 3:
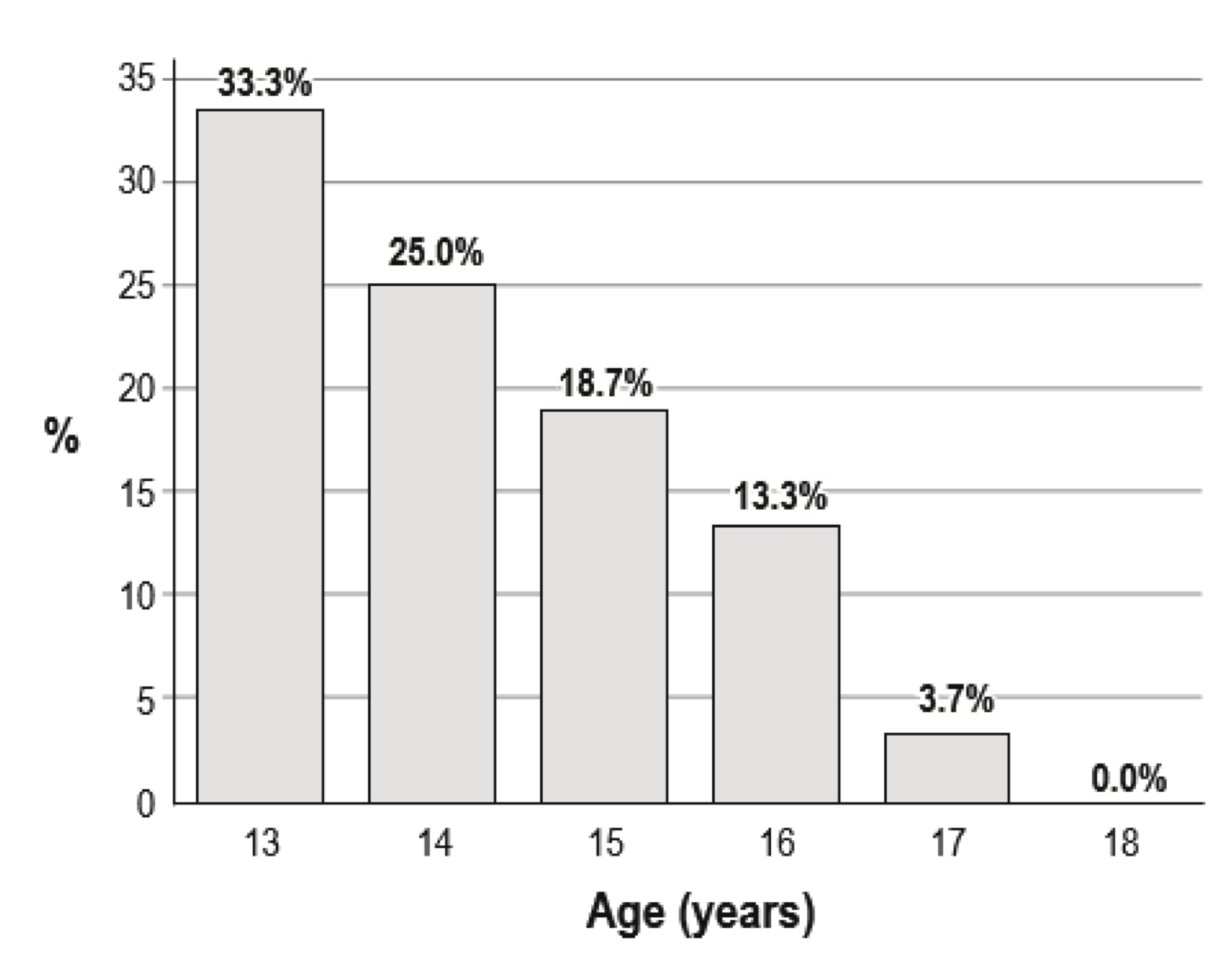
Through the teenage years, a parent is less likely to be setting a bedtime for their child (Graph 4). Adolescents with parent-set bedtimes on school nights reported earlier bedtimes on school nights, more sleep on school nights, less fatigue, and had less trouble maintaining wakefulness. (4) Research has shown earlier parent-set bedtimes were associated with more sleep, as well as a lower risk of depression and suicidal ideation than parent-set bedtimes that were either late or non-existent. (5)
Graph 4: The percentage of adolescents with a parent-set bedtime from ages 13 to 18 years:
- Hysing, Mari, et al. “Sleep and use of electronic devices in adolescence: results from a large population-based study.” BMJ open 5.1 (2015): e006748.
- Branum, Amy M., Lauren M. Rossen, and Kenneth C. Schoendorf. “Trends in caffeine intake among US children and adolescents.” Pediatrics 133.3 (2014): 386-393.
- Short, Michelle A., et al. “Time for bed: parent-set bedtimes associated with improved sleep and daytime functioning in adolescents.” Sleep 34.6 (2011): 797-800.
- Gangwisch, James E., et al. “Earlier parental set bedtimes as a protective factor against depression and suicidal ideation.” Sleep 33.1 (2010): 97-106.